Presented my 1 Button/Zio correlation analysis research to the weekly Open Humans self-research chat. The comments and feedback were excellent. Here are some images from my slides:
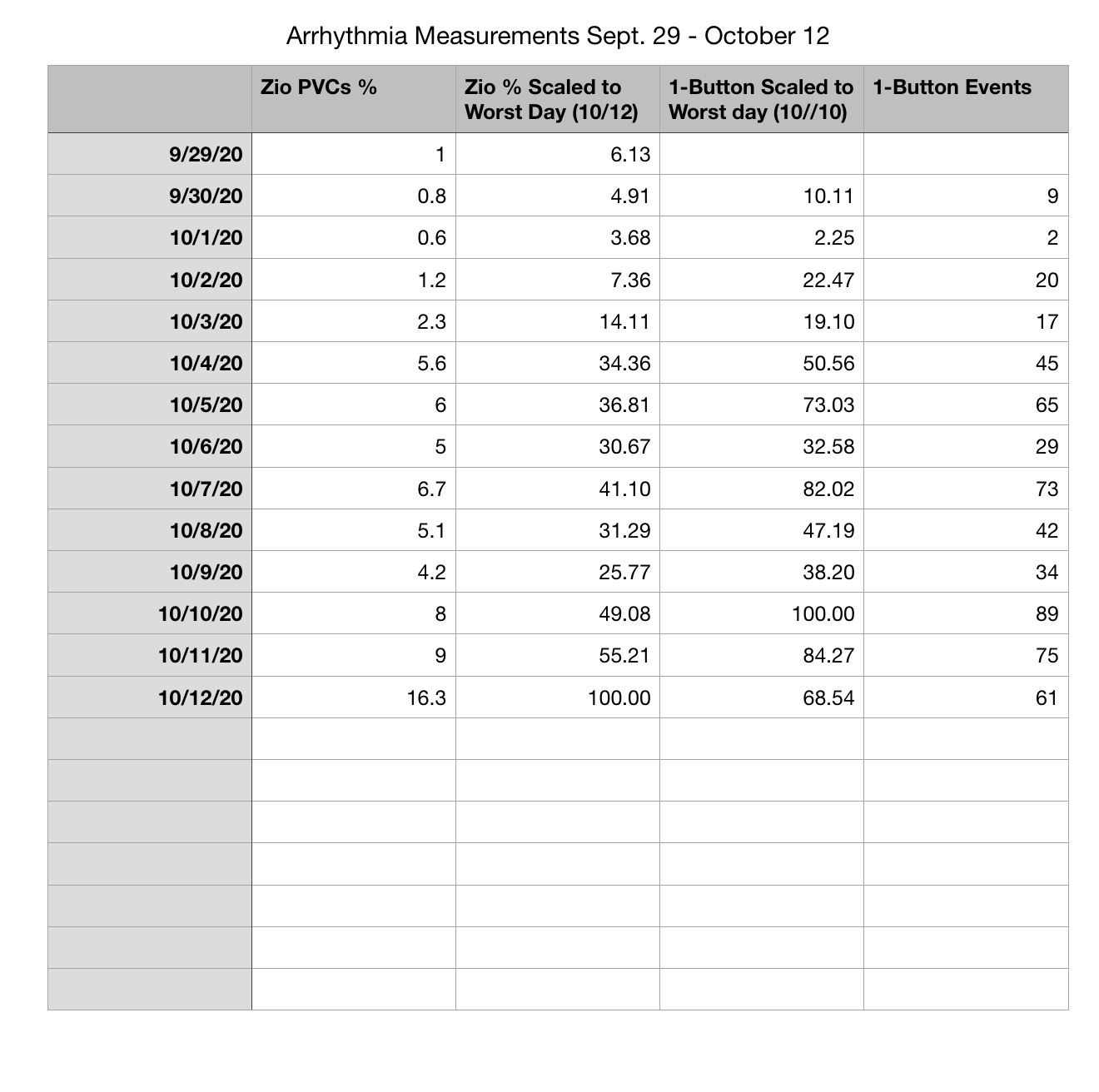
Zia and 1-Button Arrhythmia Events Table:
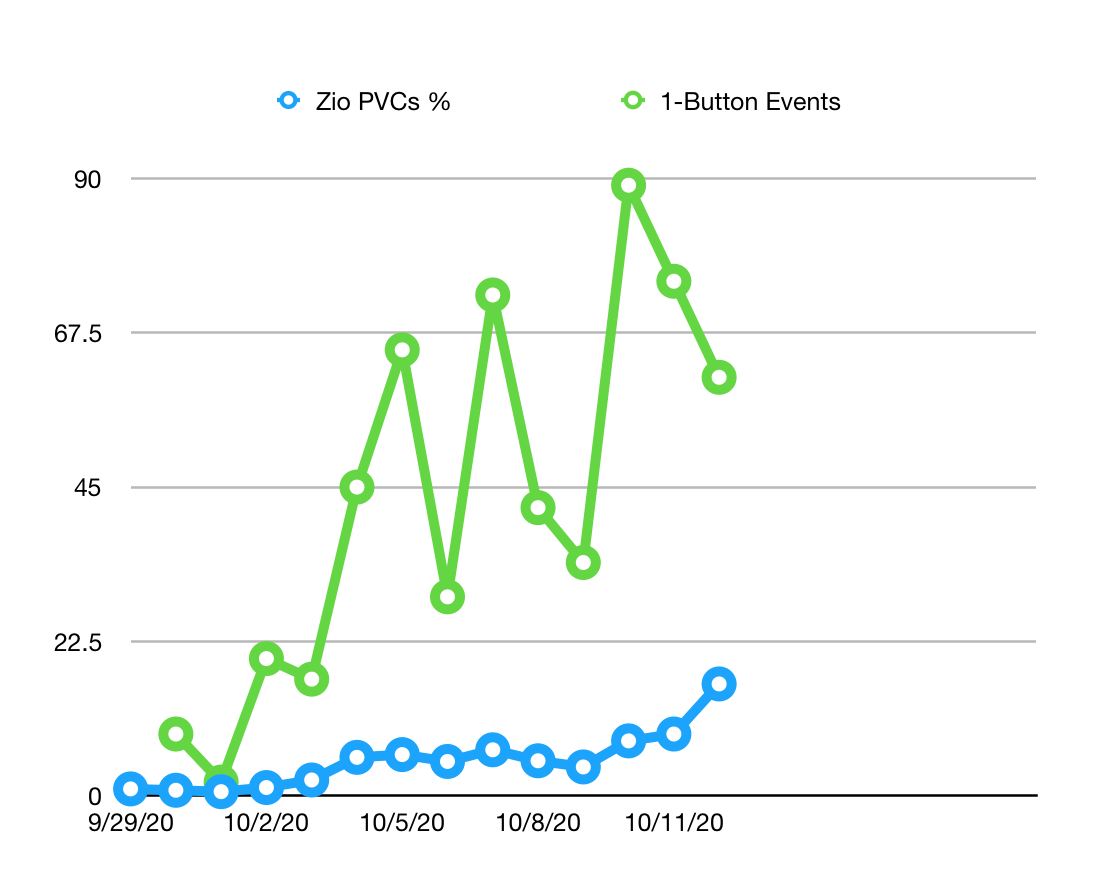
Graph of the Zio % vs 1-Button Events:
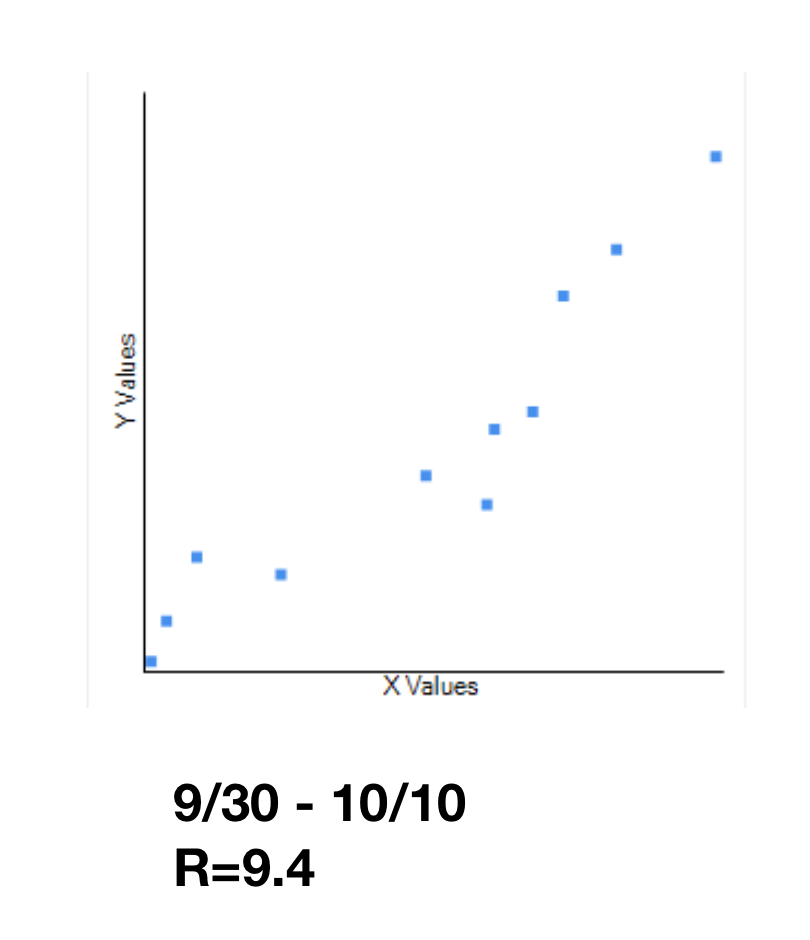
Graph of the Zeo % vs 1-Button Events Scaled to Worst Day:
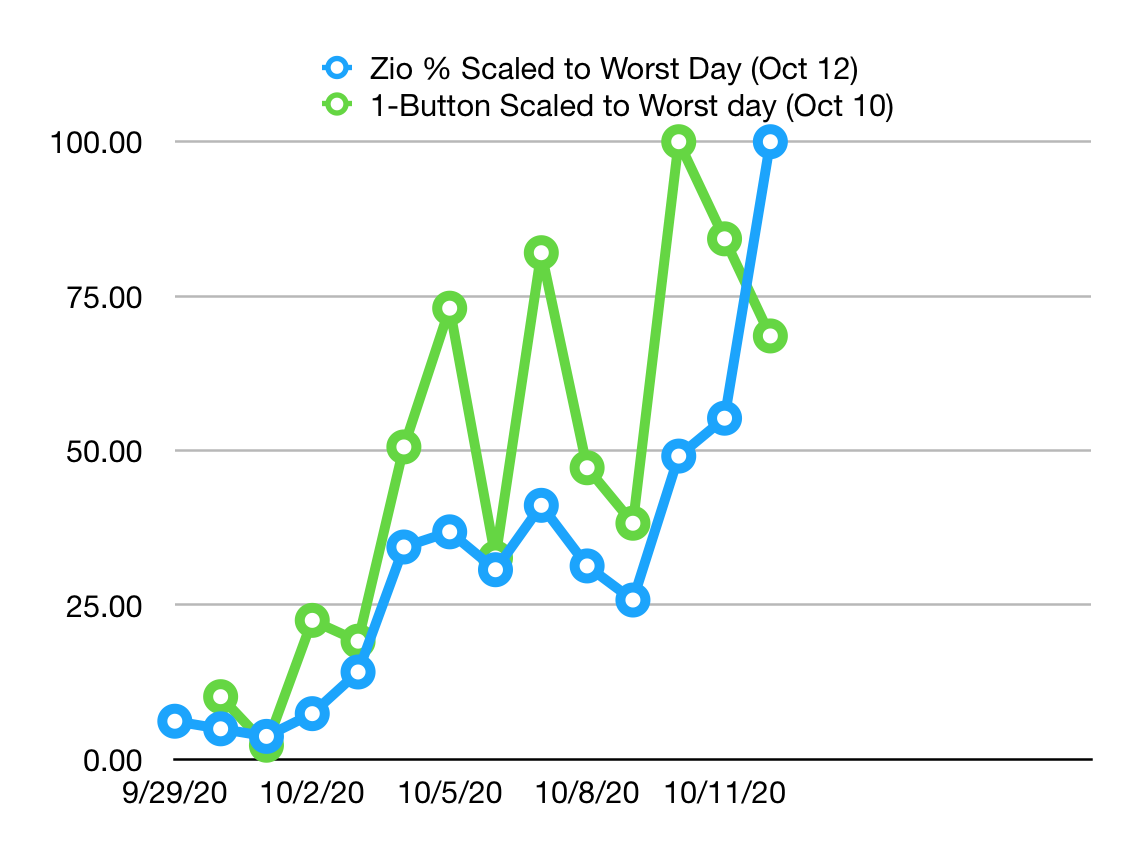
The correlation is clearly worse on the days with the highest values. This may be because I stop pressing the button at the upper range of events, just lumping the whole period together as “very bad.” Also, as mentioned last week, there may be some influence of events at night: Zio reports, but I don’t press while sleeping.
Using all the measurement days, I see a moderate correlation of 7.4:
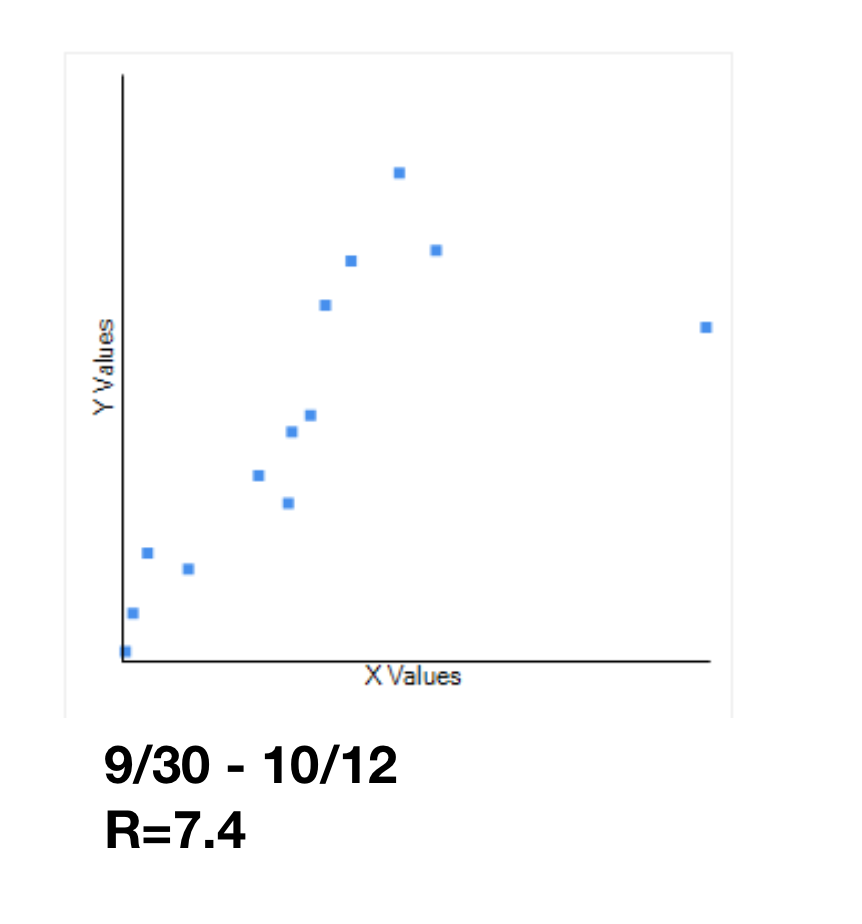
However, when I assess the correlation on the days where the Zio measurements are <50% of the worst day (10/10), the correlation is very strong: R=9.4
On a suggestion from @gedankenstuecke I may do one more additional test, setting a range of “waking hours” and checking the result. This could help tease out how much of the difference is attributable to the Zio being able to record data when I’m asleep. However, this could be a bit tricky, since I don’t go to sleep at the same time very night. And since my results are generally reassuring, it may not be worth it.
There was much discussion of interventions in the meeting. Afterwards one of the participants, Dave Blackwell, sent me this link from the blog of Dr. Anthony Pearson (aka the Skeptical Cardiologist). Pearson calls out a number of factors I believe are influencing my PVCs, including caffeine, sleep, and stress. I’m going to move on to some intervention tests in the next weeks.