Renewed PVCs after late night and Thanksgiving meal. These doses are becoming frequent enough that I’ll stop making a separate log entry for each one, and keep them on a separate list.
12.5 mg metoprolol at 11:30 pm on November 26
Renewed PVCs after late night and Thanksgiving meal. These doses are becoming frequent enough that I’ll stop making a separate log entry for each one, and keep them on a separate list.
12.5 mg metoprolol at 11:30 pm on November 26
This is clearly a transition phase in my project. Some things from the last 2 weeks:
Operational: Small details matter. I knew this already but somehow I have to relearn it with every project. I thought it was sort of dumb to enter every Metoprolol dose in the Project Log here, knowing that new forum entries generate email and new post updates to everybody who is following a topic, unless they mute them. I want to have my project be public, but I don’t want to generate excessive notifications. So I switched to tracking my medication in a separate sheet to update here more intermittently. Bad idea. Now I had two different notebooks going, and my routine was interrupted, and I lost some confidence in my notes overall. The good thing about using a project log here is that my updates are time stamped on the forum, and I have forum moderation as part of my work routine, so this helps with the cadence of the project. Lesson: Keep it simple. How many times will I outsmart myself before I just capitulate? I’m moving all my notes back here. If anybody is getting notifications who doesn’t want them, just adjust these in your forum settings.
Physiological: The metoprolol continues to work very well in reducing the PVCs, but I had a couple of odd symptoms that occurred for the first time last week. The first symptom was a kind of “brain buzz” like an electric shock in the back of my skull, not very painful but very odd and disturbing, followed by a slight headache and feeling of disorientation that lasted about an hour. The second was a strange reaction to cold that caused my toes to turn white and then red and swell up. This lasted in its severe form about two hours after working outside and then subsided over a couple of days. I didn’t find anything useful about the brain buzz, but I did locate some research on the feeling in my toes once my primary care NP talked it over with me and introduced me to the right search term: Raynauld’s syndrome. He described this as a rare but not unknown side effect of beta blockers. I did find some published reports of this, including a relatively recent (2016) meta-analysis: Peripheral vasoconstriction induced by β‐adrenoceptor blockers: a systematic review and a network meta‐analysis. My symptom wasn’t too bad, just worrisome, and I decided not to let it stop me from getting the benefit of the metoprolol for now.
In my reading on metoprolol and other beta blockers, it looks like there is some rebound effect associated with using the drugs. I haven’t analyzed my data yet to see if PVCs are worse in some window after a series of doses, but there’s no question that they are reduced in the 6 hours or so after I take a dose and then come back some time after. Therefore, for my next phase of the project, I’m going to change my dosing. Rather than taking 12.5 mg whenever the PVCs become severe, I’m going to take 12.5 every morning and another 12.5 dose 12 hours later. I think this will turn out to be about 6 am/6 pm, but let’s see.
For the sake of having everything in one place, here are my doses since November 28 (all 12.5 mg):
November 28 6:18 am
November 29 1.00 pm
December 2 11:55 pm
December 6 5:15 am
Finally: the bad news. I had some device issues that caught up with me yesterday, when I found that I’d lost all my data from December 6 to December 10. There had been an issue in the original firmware resulting in data loss when the device was out of power. The current 1-Button uses so little power that it doesn’t need to be charged very often, and I completely got out of the habit of charging it. AND, I never updated to the latest firmware over the summer when the data loss issue was fixed. So, on the evening of the 9th, I ran out of power, and lost my data going back to December 6, when I last connected it. I have now updated the firmware and come to terms with my loss. I did curse though.
Some additional notes:
Painful toes started December 5, mostly resolved December 6
December 6 left the device where I couldn’t get to it in the morning. Many presses unrecorded. Estimate: 30 presses between 4 am and 6 am. PVCs diminish starting around 5:45 am. Now 6:35 am and no PVCs.
December 6 12:30 pm after coaching soccer, PVCs ramping up again. I can’t remember if I took a second Metoprolol dose, my protocol says I should have but I failed to note it.
Conclusion: Since my data is missing December 6-10 and I had possibly one missing metoprolol dose during this time, and since I’m changing my protocol starting today, I’m going to mark those days as a transition time between project phases. The next phase will be: regular cadence of metoprolol dosing. My positive expectation is: My PVCs will drop to a manageable level and stay there without these regular increases in severity. I won’t have renewed symptoms that could be side effects. I’ll find it easy to manage routinely. My concerns are: I’ll have new symptoms that could be side effects, I’ll miss doses and find them hard to record regularly, I’ll develop a tolerance to the drug and have to increase my dose, I’ll have to stop the drug due to new symptoms and this will produce problems due to withdrawal.
Let’s see what happens.
Since you mentioned taking vitamin D: Apparently, vitamin D can trigger heart palpitations…
Thanks Eric, that was an interesting article. Some time ago I cut my vitamin D supplement from 1000 IU down to the amount in my multivitamin, 600IU. This seems pretty small compared to Jeff Chan’s case.
I’ve got almost a full month of data since starting the metoprolol. I haven’t taken a close look at it yet. Maybe worth stating some expectations before I do:
I think I’ll see that the metoprolol almost immediately improves the PVCs, with a decrease within 30 min.
I don’t think that my propensity to have PVCs has decreased. That is, I think I’ll see a rhythm of increasing PVCs as the dose wears off, and then decreasing after medication. This is so reliable that it serves as a reminder to take my medication; I notice increasing PVCs (and button presses), look at the clock, and realize I’m about 12 hours out from my last dose.
I’ve had a couple of minor data logging issues (misplaced the 1-Button for few hours, left it behind one day); otherwise have recorded the PVCs as usual. Will look at the data after the end of the month.
You can go to https://sci-hub.se and enter the exact name of paper: “Relation Between Ventricular Premature Complexes and Incident Heart Failure” and you can read full text. You can read more about this wesite here. Works fine for almost all paid articles. If website is blocked - just use vpn. After i bought few articles and found them not useful, i’ve decided to read them here at first and pay only for useful ones.
I’m doing some more arrhythmia tracking now. For the last month I’ve been making observations of arrhythmia events using the new(ish) version of the OBT.
First, an update. Looking back over my notes, it appears I stopped reporting here around May 2020. Work caught up to me, and though I continued to track both Metoprolol, cold toes, and arrhythmia episodes, I didn’t report my results on the forum.
For a while in December 2020 I took Metoprolol succinate (Toprol XL) 2x daily.
I went through a number of different trial-and-error type tests, but used my arrhythmia episode data to guide me. I didn’t like the M succinate daily because my resting heart rate dropped very low (for me) at night, and I sometimes woke up feeling short of breath. My regular resting heart rate when not on a beta blocker is 57-59, but it had gone down to 54-56. Doesn’t seem like a huge difference, but it was noticeable and not always pleasant. I also had problems with cold toes and seeming loss of circulation. So I wasn’t doing too great.
Here you can see me struggling to get the arrhythmia’s under control:
The big spike in October/November coincides with a bunch of stress, including an absolutely horrible fire season in Northern California. On November 18 I started the Metoprolol succinate, and after a data gap due to not carrying my OBT from December 1 to December 6 I switched to Metoprolol tartrate as needed. You can see I was still doing pretty badly through February 2021.
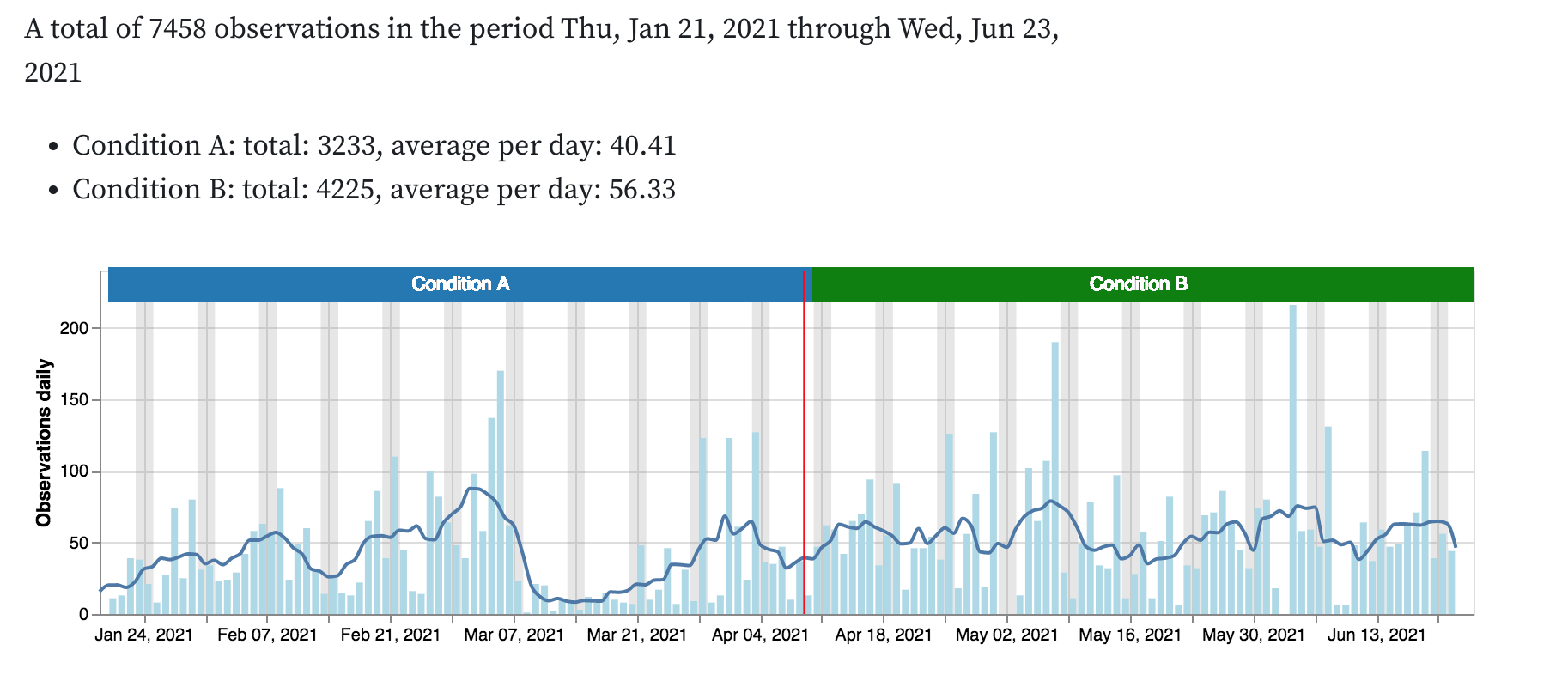
I decided during this period to do a comparison of the two forms of Metoprolol:
You can see that when I took the M succinate daily I had an average of 40 button presses per day. When I took the M tartrate I had 56. There’s a clear winner here.
But all was not well. When I returned to a daily dose my heart rate dropped even lower, 53-54. My toes were often numb. I woke up out of breath. And I was still struggled with arrhythmias, a few times pressing the button over 100 times in a day. For me, that’s a very bad day. When I returned to the short-acting M tartrate my heart rate came back up and I felt better overall, even though I still had many bad days and and significantly more button presses.
Also, during the first period I took 135 doses of M succinate. During the second period I took only 23 doses of M tartrate: I was now taking about a fifth as much medication.
What next? I finally decided to take the advice of everybody who knows something about PVC type arrhythmias and cut down on my caffeine. At first I cut from two cups of coffee per day to one, and then from one to half. I continued to take the M tartrate as needed, and paid special attention to taking it as soon as I noticed arrhythmia’s ramping up. If I felt one or two, I didn’t worry. But if I found myself pressing the button three or four times I didn’t hesitate, I took the Metoprolol.
And what do you know, the common sense recommendation everybody was handing me, plus vigilance with medication — it worked.
Here’s a snapshot from later in 2021. (My data files are badly organized, this one happened to be handy and I don’t want to delay getting this up to fish around.)
This chart shows that in October and November 2021 don’t have a single day with more than 50 button presses, and most are under twenty. I still took the M tartrate as needed, and I gained confidence that I wouldn’t have horrible days very often. At some point in late 2021 or early 2022 I accidentally put my OBT through the washing machine, and it wasn’t a crisis, because I’d learned what I needed. Since then, I’ve slowly started drinking more coffee, and still don’t have vary many bad days. For the last month I haven’t had any days with over 20 observations. That’s good.
I’m much less panicked about the arrhythmia than I was three years ago, but I still do have periods where they return and bother me. Any strong emotional stress, and they’ll activate. Interestingly, they seem to respond to the same triggers as my essential tremor, which is also relatively under control but sometimes shows up when least wanted. Both phenomena are thought to be triggered by the same sorts of things: coffee, emotional stress, lack of sleep.
Since coffee had such a dramatic effect, I’ve started to be curious about how my meals and snacks affect all these reactions. If I squint at my arrhythmia data, it seems to be more likely that I’ll press the button around mealtimes. This is chart organized by time of day, covering the same recent period as the daily count, above.
Starting this weekend, I’m going to be wearing a Freestyle Libre glucose monitor provided by Nutrisense through their support for a group self-research project I’m participating in. I’ll be interested to see if I notice any pattern linking OBT presses for arrhythmia with blood glucose levels.
How do you track stress?
Can try to use two buttons?
What measures do you take to weaken stress?
You probably already read it
Anxiety May Be The Real Cause Of Your Arrhythmia
I don’t track my stress, because I’ve never figured out the right proxy measure to trigger a button press. However, even without formal records, I’m certain that sudden stress is one of the triggers. If I have a sudden stress I often feel the arrhythmias right away, within a second or two. Interestingly, it is only a sudden stress that will do it. I can be working through a stressful challenge, whether a physical workout or some thorny interpersonal issue, and be arrhythmia free, but if I turn around and notice the rice has boiled over on the stove, I might get an attack.
Because the arrhythmias can be triggered by random events, I’m actually trying to reduce the “propensity to have arrhythmias.” This is similar to the tremor. The tremor is positional, it occurs when my hands are making fine motions with some force, like holding a full cup by the handle. Since I have to make the implicated movements in order to measure the tremor, I came up with the idea of “tremoriness” to name the phenomenon I was measuring with my protocol.
Sensor applied this morning at about 11:00 am. Really tempted to track what I eat but resisting the temptation since I know it will be distracting and I’ll eventually fail anyway.
2022 On our territory was the year of the final collapse of hopes, the collapse of illusions, losses.
Now the trend to increase the strength of different stresses.
Old methods of protection against stresses are no longer working, need to try new ones.
Health noticeably worsens from many stresses. This is important for so many.
The beginning of arrhythmia coincides with the beginning of the pandemic. Is it right?
How did you survive the storm?
Does this include “intentional” sudden stress (like a cold shower, or sudden events in a movie)?
Health noticeably worsens from many stresses.
I do think more stress = more arrhythmia generally, but they sometimes worsen when I don’t think I’m especially stressed.
The beginning of arrhythmia coincides with the beginning of the pandemic. Is it right?
No, it has been happening since about 2016.
How did you survive the storm?
We survived, though there was a power outage, and now there is another one!
Does this include “intentional” sudden stress (like a cold shower, or sudden events in a movie)?
Typically no. An argument, a spilled drink or other minor mishap, a noise that wakes me up (like if a car alarm goes off at night) , or raising my hand to speak in a formal setting where I don’t know people well are all typical triggers.
I was actually in the hospital last month for another heart attack.
With my heart attacks I have picked up PVCs (premature ventricle contractions), and I am an a lot of heart meds.
While I was hooked up to my continuous ECG, I noticed if I calmed myself enough I could set off the bradycardia (heart rate too slow) alarm (or if I genuinely just relaxed without thinking).
I wouldn’t mind being able to access my own data (the full 12 leads-10 contact version). I can contribute to collecting PVC and bradycardia data pretty regularly, lol.
I found that I couldn’t access my data from the Zio monitor my cardiologist prescribed. I had to hand copy the data from the PDFs.
Sorry to hear about your heart attacks!
That is the same issue that a group of people on a hackathon(currently ongoing) with me had with Kardia Mobile.
I had an iRhythm of some sort as well, I think it was a Zio. The data was sent to me cardiologist to read.
Patient empowerment scares some doctors because they don’t want a lot of people overloading the system. But I think the reactions of people are varied and with good design we can get the metrics (like false positives) down significantly.
Blood pressure machines can be inaccurate, but its still recommended for people to have.
Hi Agaricus,
Some thoughts:
You mentioned cold toes and I am wondering if it is a blood oxygen issue or your body responding to a threat by moving blood flow to the interior. Would monitoring toe temperature and PulseOx at the same time give a clue? I am assuming the pulse would compensate for changes in blood flow but I don’t know if it is possible to get their Automatic Gain Control (AGC) numbers out of the unit while it is computing % oxygen.
Also wondering if the arrhythmia is driven by an electrical signal or a chemical signal to your heart. When I was playing around with HRV measurements I noticed that my beat to beat variation was fairly noisy. It seemed to go sinusoidal when I was doing controlled breathing. Is it possible to detect the start of your arrhythmia on a beat to beat heart rate plot (when doing controlled breathing) and calculate the delay time between the disturbance and the start. I am thinking that electrical signal causes would be much faster than chemical signaling.
Is the magnitude of the arrhythmia event linearly related to the magnitude of the disturbance (say loudness of a car alarm)? Does knowing a noise is coming diminish the number of events?
Good luck.
uECG from ukraine, an open source device was designed in a hackathon. only 2 lead patch. I wore it for a while. Lots of poor signal but when the signal is poor its usualy obvious so what is needed is an app that can remove bad data and aggregate for useful info. https://www.tindie.com/products/ultimaterobotics/uecg-small-open-source-wireless-ecg-sensor/